
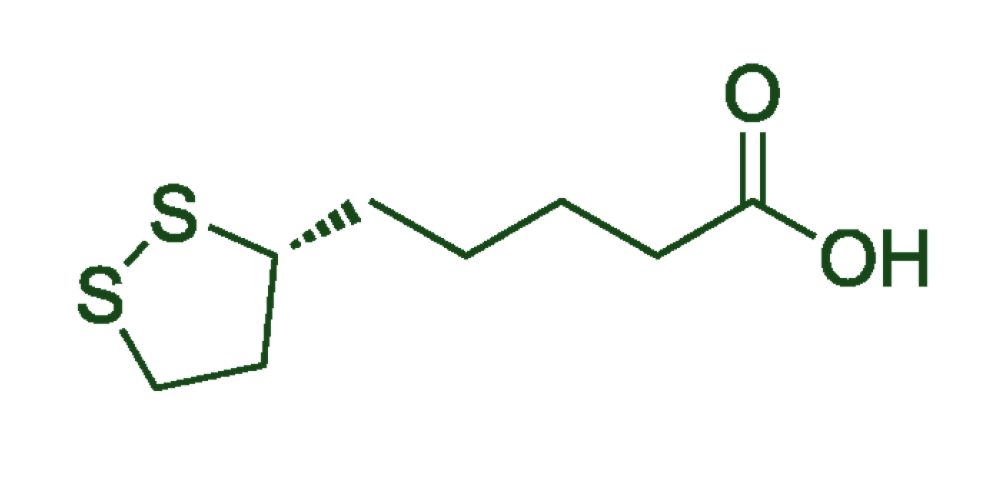
R-DLA
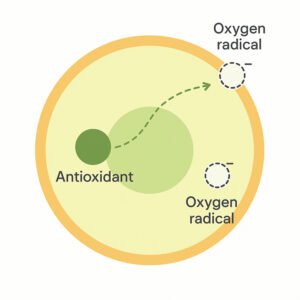
Maintains molecular structure, including two critical electrons needed to penetrate cells
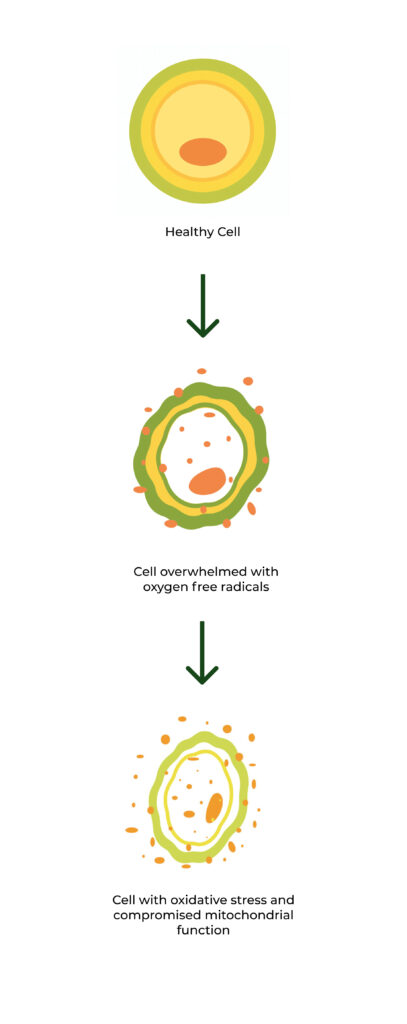
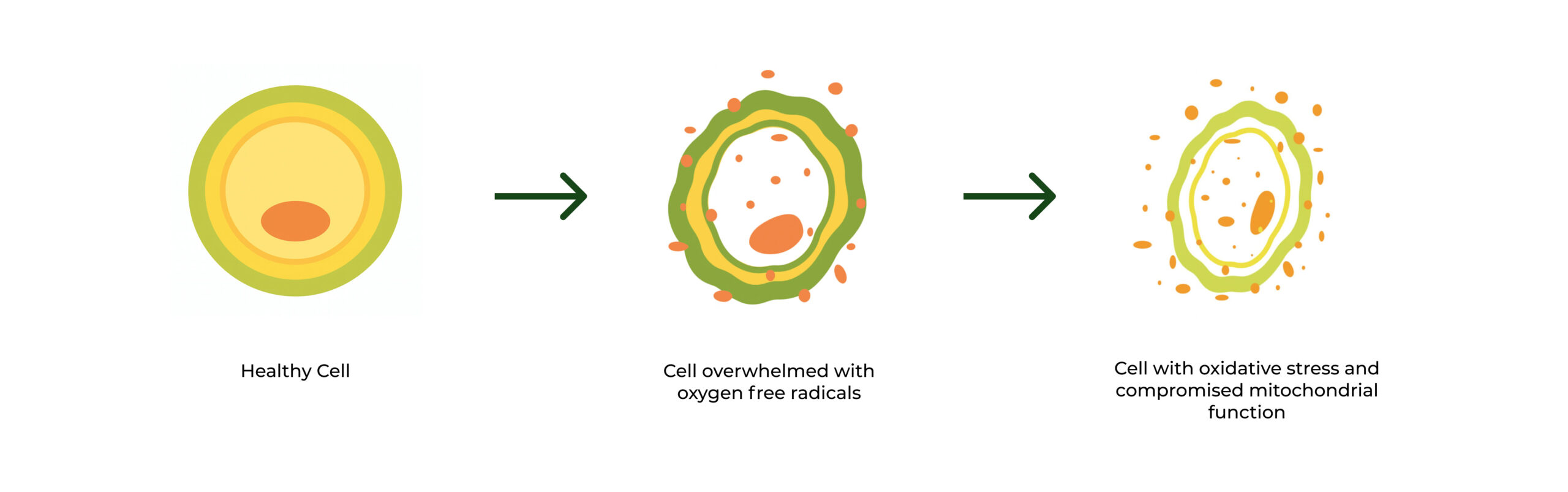
Directly neutralizes and eliminates free oxygen radicals including hydrogen peroxide and superoxide
Provides targeted support to the mitochondria in cells to boost production of glutathione and cellular energy for better resilience
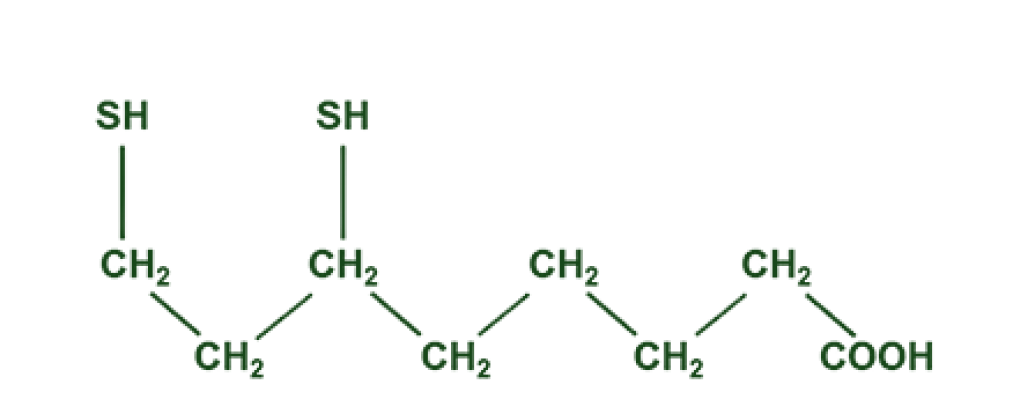
ALA
Lacks the electrons needed to neutralize
hydrogen peroxide and other damaging
oxygen radicals.
Cannot directly neutralize oxygen radicals. Must "steal" electrons from other molecules in the cell. This can cause worsening oxidative stress.
Can provide general support to the body's natural
antioxidant system for people who can tolerate the oxidative stress caused by ALA.
